Please refer to the individual studies listed below to learn more about recruitment. Each trial includes details of inclusion and exclusion criteria – namely, who can participate in each trial based on the time since stroke, mobility, and other factors.
To learn more about becoming a trial participant, please contact info@canadianstroke.ca
CAMAROS
Canadian Maraviroc Randomized Controlled Trial To Augment Rehabilitation Outcomes After Stroke
Dr. Sean Dukelow, University of Calgary
- Individuals within 5 days and 8 weeks of stroke who are experiencing hemiparesis requiring inpatient rehabilitation.

ORDER – Pilot
Optimizing Recruitment to Drive Equitable Research opportunity in stroke rehabilitation trials in Canada.
Dr. Ada Tang, McMaster University
Dr. Adria Quigley, Dalhousie University
- All individuals eligible for the CAMAROS trial will be eligible for the ORDER study.

TRAIL
TeleRehabilitation with Aims to Improve Lower Extremity Recovery Post-Stroke
Dr. Brodie Sakakibara, University of British Columbia Okanagan
Dr. Ada Tang, McMaster University
- Individuals within 12 months of stroke who are experiencing lower extremity impairment.
- VIRTUAL: British Columbia, Manitoba, Ontario, and Nova Scotia residents.

V-PASE
Virtual Physical Activity Seated Exercise Study
Dr. Janice Eng, University of British Columbia
- Adults living with stroke for more than 6 months and have a mobility impairment (e.g. walking difficulties that require a walking device in outdoor spaces or large indoor areas).
- VIRTUAL: British Columbia, Saskatchewan, Manitoba, Ontario, and Nova Scotia residents.

ICBT
Internet Delivered Cognitive Behavioral Therapy
Dr. Swati Mehta Lawson Health Research Institute
Dr. Robert Teassel, St. Joseph’s Health Care London
- People who have had a stroke and would like to improve their emotional well-being.
- VIRTUAL: Across Canada.

RESTORE
Robot-Enhanced Stroke Therapy Optimizes REhabilitation
Dr. Sean Dukelow, University of Calgary
- Individuals experiencing a recent first stroke who are experiencing an upper extremity impairment.
- Calgary, AB and Kingston, ON.

EMPOW-HER
Exploring Methods to improve Participation Of Women in clinical trials to Help Enhance stroke Recovery research
Dr. Mark Bayley, UHN Toronto Rehabilitation Institute
- The CanStroke Recovery Trials research team and men and women post-stroke.

VIPERS
VIsionand Proprioception Evaluation with Robotics after Stroke
Dr. Sean Dukelow, University of Calgary
- Individuals at timepoints 1, 6, 12, and 26 weeks post-stroke.
- Calgary, AB, Toronto, ON, Kingston, ON, and Quebec City, QC.

MODEX
Modafinil and Exercise for Post Stroke Fatigue
Dr. Mark Bayley, UHN – Toronto Rehabilitation Institute
- Individuals with fatigue over 3 months post-stroke.
- VIRTUAL: Calgary, AB, Vancouver, BC, Toronto, ON, and Halifax, NS.

ANIMATOR
brain controlled robotic arm rehabilitation for stroke
Dr. Sean Dukelow, University of Calgary
Dr. Janice Eng, University of British Columbia
Dr. Mark Bayley, UHN – Toronto Rehabilitation Institute
- Individuals more than 6 months post-stroke with severe arm impairment.
- Calgary, AB, Toronto, ON, Vancouver, BC.

STRIVE
STroke Recovery wIth Virtual rEality
Dr. Sean Dukelow, University of Calgary
- Designing a Virtual Reality module for people with post-stroke aphasia.
- Conducting a pilot study for individuals less than 6 months post-stroke with expressive aphasia.
- Calgary, AB.


Dr. Sean Dukelow is the study Principal Investigator.
Canadian Maraviroc Randomized Controlled Trial To Augment Rehabilitation Outcomes After Stroke: CAMAROS
Description:
After stroke, the combination of progressive skills practice in an adequate dose, exercise for fitness augments motor and cognitive outcomes. However, sensorimotor and cognitive improvements often plateau after 12 weeks. There is an urgent need to find novel methods to drive recovery and lessen limb paralysis. Drugs that might enhance learning or neural repair, as well as other molecular and synaptic adaptations that occur during skills training and fitness exercise, might extend that recovery curve. Several very recent preclinical experiments and observational studies in patients after stroke suggest that the commercially available medication, Maraviroc, may augment skills learning during rehabilitation training especially during the first three months after onset, by acting on unique molecular components for novel learning.
The CAMAROS trial is a randomized, placebo-controlled, blinded phase II trial evaluating the efficacy of coupling Maraviroc (Celsentri) with exercise rehabilitation across multiple Canadian sites in 120 stroke participants. Participants will begin their participation within 8 weeks of stroke onset. Both groups will receive an exercise program in addition to standard of care rehabilitation, but only one group (the intervention group) will receive the active drug Maraviroc.
Participants will be evaluated using physical assessments, cognitive assessments, and using wrist and ankle activity sensors at baseline, after 4 weeks of taking the drug/placebo, after 8 weeks of taking the drug/placebo, and at 6-months post-stroke. While enrolled in the study, participants will be required to take part in an 8 week, daily exercise program. Participants will also perform a short motor learning assessment at each formal assessment and again within 24 hours of each formal assessment (initial test and 24-hour retention test).
Sites involved:
- Vancouver, BC
- Kelowna, BC
- Calgary, AB
- London, ON
- Toronto, ON
- Kingston, ON
- Windsor, ON
- Quebec City, QC
- Halifax, NS
- Charlottetown, PEI
Principal Investigator:
Dr. Sean Dukelow, MD, PhD, University of Calgary/Hotchkiss Brain Institute
Other Investigators:
Vancouver, BC:
Drs Janice Eng, Courtney Pollock, Jennifer Yao
Kelowna, BC:
Drs Brodie Sakakibara, Aleksander Tkach
Calgary, AB:
Drs Sean Dukelow, Gentson Leung
London, ON:
Dr. Robert Teasell
Toronto, ON:
Drs Mark Bayley, Bradley MacIntosh, Sandra Black
Kingston, ON:
Drs Stephen Scott, Benjamin Ritsma
Windsor, ON:
Drs Jennifer Voth, Nathania Liem
Quebec City, QC
Dr. Catherine Mercier
Halifax, NS:
Drs Marilyn Mackay-Lyons, Anita Mountain
Charlottetown, PEI:
Drs Trish Helms-Neima, Nathanial Heinrichs
Target population:
Individuals within 5 days and 8 weeks of stroke who are experiencing hemiparesis requiring inpatient rehabilitation.
Recruitment:
The trial is currently recruiting participants. Target recruitment n = 120.
Eligibility:
Inclusion Criteria
- Primary ischemic anterior circulation stroke
- age ≥18 years
- at least 5 days after stroke but within 8 weeks of stroke on the date of medication (maraviroc or placebo) start
- hemiparesis requiring inpatient rehabilitation
- at least one of the following:
- some shoulder abduction, with gravity eliminated and visible extension in two or more digits
OR - visible hip flexion or extension
- some shoulder abduction, with gravity eliminated and visible extension in two or more digits
- assistance available for daily rehabilitation training practice and for transportation when needed
- adequate language skills to understand the Informed Consent and retain information during daily therapies
Exclusion Criteria
- pre-stroke modified Rankin score ≥ 2
- limited resources or illness that will not enable a return to living outside of a facility
- history of dementia
- history of hepatitis or elevated hepatic transaminases or bilirubin
- history of renal insufficiency or creatinine clearance (eGFR) < 60mL / min / 1.73m2
- cancer or other chronic illness that makes 1-year survival unlikely or will detract from the ability to carry out exercise and skills practice
- existing pre-stroke serious disabling disease (e.g., Parkinson’s disease, severe traumatic brain injury, amputation)
- seizure related to stroke
- acute or chronic epilepsy
- currently taking any of the following anticonvulsant medications:
- Carbamazepine, Phenobarbital, or Phenytoin
- pregnant, breastfeeding, or positive test for pregnancy at baseline
- women of childbearing potential who are not using one highly effective form of contraception or two forms of effective contraception
- known HIV positivity
- currently taking any of the following antifungal and/or antibacterial medications:
- Ketoconazole, Itraconazole, Voriconazole, Rifampin, Clarithromycin, or Rifabutin + Protease Inhibitor
- currently taking St. John’s Wort
Subgroup Stratification Criteria
For Upper Extremity Group:
Minimum Ability: Medical Research Council (MRC) grade >1 for shoulder abduction AND MRC grade >1 for finger extensor on at least one digit
Maximum Ability: Upper Extremity Fugl-Meyer Assessment Score >56
For Lower Extremity Group:
Minimum Ability: requiring a 2-person assist
Maximum Ability: walking speed <0.8m/s

Drs Ada Tang and Adria Quigley, pictured here, are the study leaders.
Description
Research studies in stroke recovery can help us better understand effective rehabilitation treatments to help reduce the burden of stroke.
Some groups of people however are often not as well represented in studies. For example, it is more common for men to take part in stroke research than women, and people with aphasia (a language impairment commonly seen after stroke) are often excluded from studies. Also, deciding whether to even take part in a research study can be difficult and overwhelming, especially in the early days after stroke, leaving many people to decline to participate.
Research has shown that women experience different barriers to participating in stroke research than men. This means that research findings, and the decisions made during stroke care based on these findings, may not reflect the true stroke population.
As researchers, we need to find better ways to help support groups like women and people with aphasia to participate in stroke research, so that study findings will better represent people living with stroke. In short, we need research on how to do research better.
With our pilot study, “Optimizing Recruitment to Drive Equitable Research opportunity in stroke rehabilitation trials in Canada” (ORDER-Pilot), we are taking the first steps in helping us understand how to optimize efficiency and quality in conducting clinical trials, and recruiting more diverse samples that are representative of the broader stroke population.
ORDER-Pilot is a ‘study-within-a-trial’, nested within Canadian Maraviroc RCT to Augment Rehabilitation Outcomes after Stroke (CAMAROS ; ‘host trial’). It will test the use of a supported, women-centred and aphasia-friendly recruitment and enrollment process for CAMAROS.

ORDER-Pilot also includes a substudy using survey and interviews to understand participants’ experiences of being approached by researchers to participate in CAMAROS.
Using a ‘study within a trial’ design, we are addressing important research gaps about the best tools for recruitment into trials, and understanding process factors such as participants’ perceptions of recruitment methods.
If ORDER-Pilot is feasible and potentially effective as a recruitment strategy for CAMAROS, we will have pilot evidence to support scale-up for future, larger trials on the CanStroke Recovery platform.
Sites involved
- Vancouver, BC
- Kelowna, BC
- Calgary, AB
- London, ON
- Toronto, ON
- Kingston, ON
- Windsor, ON
- Quebec City, QC
- Halifax, NS
- Charlottetown, PEI
Principal Investigators
Dr. Ada Tang, McMaster University
Dr. Adria Quigley, Dalhousie University
Other Investigators
Vancouver, BC:
Drs Janice Eng, Courtney Pollock
Kelowna, BC:
Dr. Brodie Sakakibara
Ms. Jennifer Monaghan, Patient Partner
Calgary, AB:
Drs Sean Dukelow, Michael Hill
Hamilton, ON:
Drs Jinhui Ma, Victrine Tseung
London, ON:
Dr. Robert Teasell
Toronto, ON:
Drs Mark Bayley, Susan Marzolini
Kingston, ON:
Drs Stephen Scott, Benjamin Ritsma
Windsor, ON:
Dr. Nathania Liem
Quebec City, QC
Dr. Catherine Mercier
Halifax, NS:
Dr. Marilyn Mackay-Lyons
Ms. Ferne Mardlin-Smith, Patient Partner
Target population
All individuals eligible for the CAMAROS trial will be eligible for the ORDER study, i.e. within 5 days and 8 weeks of stroke who are experiencing hemiparesis requiring inpatient rehabilitation.
Recruitment
The ORDER study is currently recruiting participants
Target recruitment n = 466
Study eligibility
Participants for the ORDER study will be all individuals eligible and approached for screening for the CAMAROS trial.
Internet-delivered cognitive behavioural therapy for persons with stroke: ICBT

Drs. Swati Mehta (left) and Robert Teassel (right) are the study Principal Investigators.
Description:
In Canada, stroke is a leading cause of adult disability. Along with the physical concerns, approximately 30% of people often experience symptoms of depression, but only 2- 3% access support. Unhelpful thoughts of never being able to go back to their life before their stroke and fear of recurring stroke can result in feelings of loss and hopelessness. If these thoughts go untreated over a long period of time, they can potentially lead to decreased quality of life and greater disability. Many of these individuals may benefit from access to mental health services, eg. cognitive behaviour therapy (CBT), that target maladaptive thoughts and behaviours. CBT is an evidenced based treatment strategy that helps patients recognize and challenge their unhelpful thoughts and behaviours that contribute to their mental health concerns. However, after stroke people often go untreated for various reasons, such as access to specialized care, costs, rural and remote location, lack of time, or concerns about stigma related to seeking care. One way to overcome these barriers is to provide these services over the internet. Internet delivered CBT (ICBT) has the potential for reaching a much wider group of people that may have unequal access to services.
Sites Involved:
- Canada-wide (Virtual)
Principal Investigator:
Swati Mehta, PhD Lawson Health Research Institute
Robert Teassel, MD St. Joseph’s Health Care London
Eligibility:
- Participants who have sustained a stroke and would like to learn strategies to improve their emotional well-being.
- The program is tailored to those with stroke that may have mobility and cognitive impairments.
Participant requirements:
Participants will be enrolled in an online 10-week program with potential guidance from a trained mental health clinician each week over the phone or through videoconferencing.
To learn more: swati.mehta@sjhc.london.on.ca
Dr. Sean Dukelow is the study Principal Investigator.
Robot-Enhanced Stroke Therapy Optimizes REhabilitation: RESTORE
Description:
Robotics in upper limb stroke rehabilitation first garnered attention in late 1990’s. Robots were a way to 1) perform passive range of motion and reduce hypertonia (resistance to passive movement), 2) aid patients in performing movements that would not otherwise be possible because of weakness and 3) increase strength by providing resistance to movements. The first observational study focused on chronic stroke and showed that working with a simple robotic device, the MIT-Manus, could improve motor function. Many observational studies using robotics for motor rehabilitation followed. As the number and complexity of robots increased, so did study designs.
Case-control and small single centre randomized controlled trials evaluated robotic therapy versus standard rehabilitation care or sham therapy. In most studies, robotic rehabilitation proved superior to the control conditions.
The purpose of this study is to investigate two aspects of robotic therapy after stroke. One goal is to determine if early robotic rehabilitation of the upper limb (beginning 5-9 days post-stroke) is more effective than later robotic rehabilitation (beginning 21-25 days post-stroke). The other goal is to determine if higher intensity robotic rehabilitation (2 hours/day) is more effective than lower intensity robotic rehabilitation (1 hour/day).
Sites Involved:
Calgary, AB
Kingston, ON
Principal Investigator
Dr. Sean Dukelow, MD, PhD, University of Calgary, Hotchkiss Brain Institute
Other Investigators:
Calgary, AB
Dr. Sean Dukelow
Kingston, ON
Drs Stephen Scott, Benjamin Ritsma
Target Population:
Individuals experiencing a recent first stroke who are experiencing an upper extremity impairment.
Recruitment:
The trial is currently recruiting participants.
Target recruitment n = 132 stroke participant, n=24 control participants.
Study Eligibility:
Inclusion Criteria – Stroke:
- Recent first stroke (ischemic or hemorrhagic)
- Upper extremity Fugl-Meyer score 15-45
- Modified Ashworth score of shoulder/elbow less than or equal to 2
- Able to follow task instructions
- Visual acuity better than 20/50 in both eyes
- Able to give consent
- Able to commit to follow-up
Inclusion Criteria – Control:
- Aged 18 or older
- Visual acuity better than 20/50 in both eyes
- Able to give consent
- Able to complete intervention
Exclusion Criteria:
- Prior stroke or significant neurologic problem (e.g. Multiple Sclerosis)
- Pre-existing musculoskeletal injury that will interfere with active therapy
- Pre-Stroke Modified Rankin Score > 2
- Clinical evidence of Unilateral Spatial Neglect on the Behavioural Inattention Test (BIT)
- Enrollment in a concurrent clinical intervention trial
- Major co-morbid or concurrent illness such that improvement is unlikely or completion of the protocol as specified is unlikely

Drs Brodie Sakakibara and Ada Tang are the study Principal Investigators.
TeleRehabilitation with Aims to Improve Lower Extremity Recovery Post-Stroke: TRAIL
TRAIL Randomized Controlled Trial (TRAIL-RCT)
Description:
The multi-site RCT aims to compare functional mobility between stroke survivors in TRAIL, a 4-week progressive intensity and self-management support telerehabilitation program, and those in the attention-controlled stroke education program (EDUCATION). The trial also compares lower extremity muscle strength, motor impairment, functional balance, balance self-efficacy, and costs and health-related quality of life between TRAIL and EDUCATION participants.
The end goal is to inform best practices in virtual care and have widespread application in practice when access to in-person rehabilitation is not feasible, such as in rural, remote and under-serviced areas.
Sites involved:
- Vancouver
- Kelowna
- Winnipeg
- Halifax
- Toronto
- London
Principal Investigators:
Dr. Ada Tang, McMaster University
Dr. Brodie Sakakibara, University of British Columbia, Okanagan
Other investigators:
- Nova Scotia Health Authority (Halifax), site investigator Dr. Marilyn Mackay-Lyons,
- University Health Network (Toronto), site investigator Dr. Mark Bayley,
- Parkwood Institute (London), Dr. Robert Teasell,
- Riverview Health Centre (Winnipeg), Dr. Ruth Barclay & Dr. Sepideh Pooyania,
- GF Strong Rehabilitation Centre (Vancouver), Dr. Courtney Pollock.
- McMaster University (Hamilton), Elise Wiley, PhD candidate
- Patient Partner, Jennifer Monaghan
Target population for the trial:
Individuals within 12 months of stroke who are experiencing lower extremity impairment.
Recruitment:
The trial is currently recruiting participants
Target recruitment n=96 (n=48 females, 48 males)
Study eligibility:
Inclusion Criteria:
- ≥19 years of age
- ≤12 months post-stroke with lower extremity hemiparesis
- Walk ≥10 meters with or without a gait aid and without physical assistance of another person
- Tolerate 50 minutes of activity (including rest breaks)
Exclusion Criteria:
- Currently participating in formal in- or out-patient stroke rehabilitation focusing on lower extremity training
- Living in long-term care
- Severe vision or hearing loss
- Significant musculoskeletal or other neurological conditions
- Not medically stable
- Comorbidities (e.g. limb amputation), pain or other symptoms that significantly impact lower extremity
To learn more: info@canadianstroke.ca
Telerehabilitation with Aims to Improve Lower Extremity Recovery – Proof-of-Concept (TRAIL-PROOF)
The TRAIL-RCT was preceded by a proof-of-concept study, TRAIL-PROOF.
Description:
TRAIL-Proof was a feasibility study aiming to examine the feasibility of a 4-week lower extremity telerehabilitation program to improve lower extremity recovery among community-living stroke survivors across Canada. Thirty-two patients have been enrolled in the study at 5 Canadian sites.
Participants received a telerehabilitation program comprised of evidence-based exercises and self-management delivered by physiotherapist trained in telerehabilitation over videoconferencing. The program consisted of two 60-minute telerehabilitation sessions per week over the course of 4 weeks. Participants were also asked to complete at least one additional independent self-managed exercise session each week. Study participants were evaluated before the start of the telerehabilitation program and immediately after the telerehabilitation program.
Sites involved:
University of British Columbia & GF Strong Centre, Vancouver, British Columbia
Riverview Health Centre, Winnipeg, Manitoba
Dalhousie University, Halifax, Nova Scotia
Parkwood Institute, London, Ontario
Toronto Rehabilitation Institute – University Health Network, Toronto, Ontario
Principal Investigators:
Brodie Sakakibara, PhD
Ada Tang PT PhD
Other Investigators:
Mark Bayley, MD. University Health Network, Toronto
Courtney Pollock, PhD. University of British Columbia & Rehabilitation Research Program
Janice Eng, PhD. University of British Columbia & Rehabilitation Research Program
Sepideh Pooyania, MD. Riverview Health Centre
Ruth Barclay, PhD. Riverview Health Centre
Marilyn Mackay-Lyons, PhD. Dalhousie University
Robert Teasell, MD. Parkwood Institute
Sarah Park, MSc, University of British Columbia & Rehabilitation Research Program
TRAIL Publications
May 24, 2024 Associations between balance self-efficacy and virtual balance performance
Examining the association between balance self-efficacy and virtual balance performance in individuals with stroke: a cross-sectional study
Authors: Eric Huynh, Elise Wiley, Sarah Park, Brodie M Sakakibara, Ada Tang
Published in Top Stroke Rehabil. 2024 May 24:1-9. doi: 10.1080/10749357.2024.2356407. Online ahead of print.
Link to paper https://www.tandfonline.com/doi/full/10.1080/10749357.2024.2356407
March 1, 2024 Results from TRAIL Proof of Concept Study
Investigating the Telerehabilitation With Aims to Improve Lower Extremity Recovery Poststroke Program: A Feasibility Study
Authors: Sarah Park, Ada Tang, Ruth Barclay, Mark Bayley, Janice J Eng, Marilyn Mackay-Lyons, Courtney Pollock, Sepideh Pooyania, Robert Teasell, Jennifer Yao, Brodie M Sakakibara
Published in Phys Ther. 2024 Mar 1;104(3):pzad165. doi: 10.1093/ptj/pzad165.
Link to paper: https://pubmed.ncbi.nlm.nih.gov/38051660/
February 15, 2024 Qualitative study of participant experiences of TRAIL
Exploring the experiences of an exercise-based telerehabilitation program among Canadian community-dwelling adults with stroke
Authors: Elise Wiley, Brodie Sakakibara, Sarah Park, Ruth Barclay, Mark Bayley, Janice J Eng, Anne Harris, Elizabeth Inness, Marilyn MacKay-Lyons, Joy MacDermid, Courtney Pollock, Sepideh Pooyania, Robert Teasell, Jennifer Yao, Ada Tang
Published in Disabil Rehabil. 2024 Feb 15:1-11. doi: 10.1080/09638288.2024.2316772. Online ahead of print.
Link to paper https://www.tandfonline.com/doi/full/10.1080/09638288.2024.2316772
July 19, 2023 Protocol for TRAIL Randomized Controlled Trial
TeleRehabilitation with Aims to Improve Lower extremity recovery in community-dwelling individuals who have had a stroke: protocol for a multisite, parallel group, assessor-blinded, randomised attention-controlled trial
Authors: Brodie M Sakakibara, Elise Wiley, Ruth Barclay, Mark Bayley, Jennifer C Davis, Janice J Eng, Anne Harris, Elizabeth L Inness, Marilyn MacKay-Lyons, Jennifer Monaghan, Courtney Pollock, Sepideh Pooyania, Amy Schneeberg, Robert Teasell, Jennifer Yao, Ada Tang
Published in BMJ Open. 2023 Jul 19;13(7):e076723. Doi: 10.1136/bmjopen-2023-076723.
Link to paper: https://bmjopen.bmj.com/content/13/7/e076723.long
TRAIL In the News
28 March 2024 UBC Okanagan News, Virtual rehabilitation provides benefits for stroke recovery https://news.ok.ubc.ca/2024/03/28/virtual-rehabilitation-provides-benefits-for-stroke-recovery/
July 10, 2022 Vancouver Coastal Health Research Institute article, Making lower body rehabilitation more accessible to stroke patients https://www.vchri.ca/stories/2022/07/10/making-lower-body-rehabilitation-more-accessible-stroke-patients
19 January 2022 Interview with UK-based NR Times, TRAIL study brings new remote rehab potential to stroke survivors https://nrtimes.co.uk/trail-study-brings-new-remote-rehab-potential-to-stroke-survivors/

Dr. Janice Eng is the study Principal Investigator.
Virtual Physical Activity Seated Exercise Study: V-PASE
Description:
The Virtual Physical Activity Seated Exercise (V-PASE) study is a 10-week online exercise study in those living with a stroke and mobility impairment. The study has the potential to improve an individual’s balance, mobility, muscle strength, quality of life, and heart health (sugar and cholesterol levels).
The study is conducted in multiple provinces across Canada with all sessions being completed online (e.g., Zoom) in the comfort of your own home. Intensive seated exercise sessions will be delivered by a trained instructor or physical therapist and will be 60 minutes in duration and take place 3 times per week.
Who can join this study?
- Adults who have been living with stroke more than 6 months
- Live in BC, Saskatchewan, Manitoba, Ontario, or Nova Scotia
- Have ongoing walking and standing issues due to their stroke
- Use a walking device such as a cane or walker in large indoor spaces (e.g., shopping mall) or outdoor spaces, and
- Able to stand up from a chair.
Principal Investigator:
Dr. Janice Eng, University of British Columbia
Other investigators:
British Columbia – Dr. Paul Mackie | Dr. Jennifer Yao | Dr. Ben Mortenson | Sally-Anne Stelling | Dr. Courtney Pollock | Dr. Maureen Ashe | Dr. Brodie Sakakibara
Saskatchewan – Dr. Sarah Donkers
Manitoba – Dr. Ruth Barclay | Dr. Sepideh Pooyania
Ontario – Dr. Sue Peters | Dr. Mark Bayley
Nova Scotia – Dr. Adria Quigley
Target population for the trial:
Adults living with a stroke for more than 6 months and have a mobility impairment (walking difficulties that require a walking device in outdoor spaces or large indoor areas).
Access to a local blood facility for sugar and cholesterol lab work is needed. We can work with local health authorities to schedule blood work.
Recruitment:
The trial is currently recruiting patients in all Provinces listed above.
To learn more: info@canadianstroke.ca

Dr. Mark Bayley is the study Principal Investigator.
Exploring Methods to improve Participation Of Women in clinical trials to Help Enhance stroke Recovery research: EMPOW-HER
Description:
Sex differences exist in the burden of stroke and treatment efficacy, therefore equal representation in research studies is of paramount importance. However, women are under-represented in stroke research trials reducing the generalizability of research outcomes.
Therefore, we are conducting two cross-sectional questionnaire-based studies and one focus group to determine sex and gender-related factors associated with willingness to participate in stroke research studies. A retrospective review of CanStroke Recovery Trials data is also underway, to determine whether the sex distribution as well as other demographic and clinical characteristics of participants differed from that of the general diseased population.
Sites Involved:
A survey of the CanStroke research team will be sent to all current CanStroke personnel to explore their perceptions of barriers and facilitators to recruitment of women and men in clinical trials.
Respondents for the survey of people post-stroke will be recruited from 9 sources across Canada. These include in-patient and out-patient stroke rehabilitation programs, cardiovascular rehabilitation, and March of Dimes.
We will also be contacting the CanStroke Trials Recovery Platform researchers to invite them to disseminate research flyers to the patients of their studies.
Principal Investigator:
Dr. Mark Bayley, MD
Other Investigators:
Dr. Susan Marzolini
Dr. Shannon MacDonald
Dr. Urvashy Gopaul
Dr. Amy Yu
Juliana Nunes da Silva
And others from the CanStroke research team.
Target population:
The CanStroke Recovery Trials research team.
Men and women post-stroke.
Recruitment:
Recruitment is underway for the cross-sectional questionnaire of people post-stroke (target of 400 respondents).
Study eligibility:
Men and women (at least 18 years of age) having had at least one stroke (any type).
Ability to read in English.
Dr. Sean Dukelow is study Principal Investigator.
Description
VIsion and Proprioception Evaluation with Robotics after Stroke (VIPERS) will assess vision and proprioceptive impairments after stroke using eye tracking software on the KinArm Exoskeleton.
Recruitment will be underway in the Fall of 2025 from sites in Calgary, AB, Toronto, ON, Kingston, ON, and Quebec City, QC.
Dr. Sean Dukelow is the study Principal Investigator.
Canadian Maraviroc Randomized Controlled Trial To Augment Rehabilitation Outcomes After Stroke: CAMAROS
Description:
After stroke, the combination of progressive skills practice in an adequate dose, exercise for fitness augments motor and cognitive outcomes. However, sensorimotor and cognitive improvements often plateau after 12 weeks. There is an urgent need to find novel methods to drive recovery and lessen limb paralysis. Drugs that might enhance learning or neural repair, as well as other molecular and synaptic adaptations that occur during skills training and fitness exercise, might extend that recovery curve. Several very recent preclinical experiments and observational studies in patients after stroke suggest that the commercially available medication, Maraviroc, may augment skills learning during rehabilitation training especially during the first three months after onset, by acting on unique molecular components for novel learning.
The CAMAROS trial is a randomized, placebo-controlled, blinded phase II trial evaluating the efficacy of coupling Maraviroc (Celsentri) with exercise rehabilitation across multiple Canadian sites in 120 stroke participants. Participants will begin their participation within 8 weeks of stroke onset. Both groups will receive an exercise program in addition to standard of care rehabilitation, but only one group (the intervention group) will receive the active drug Maraviroc.
Participants will be evaluated using physical assessments, cognitive assessments, and using wrist and ankle activity sensors at baseline, after 4 weeks of taking the drug/placebo, after 8 weeks of taking the drug/placebo, and at 6-months post-stroke. While enrolled in the study, participants will be required to take part in an 8 week, daily exercise program. Participants will also perform a short motor learning assessment at each formal assessment and again within 24 hours of each formal assessment (initial test and 24-hour retention test).
Sites involved:
- Vancouver, BC
- Kelowna, BC
- Calgary, AB
- London, ON
- Toronto, ON
- Kingston, ON
- Windsor, ON
- Quebec City, QC
- Halifax, NS
- Charlottetown, PEI
Principal Investigator:
Dr. Sean Dukelow, MD, PhD, University of Calgary/Hotchkiss Brain Institute
Other Investigators:
Vancouver, BC:
Drs Janice Eng, Courtney Pollock, Jennifer Yao
Kelowna, BC:
Drs Brodie Sakakibara, Aleksander Tkach
Calgary, AB:
Drs Sean Dukelow, Gentson Leung
London, ON:
Dr. Robert Teasell
Toronto, ON:
Drs Mark Bayley, Bradley MacIntosh, Sandra Black
Kingston, ON:
Drs Stephen Scott, Benjamin Ritsma
Windsor, ON:
Drs Jennifer Voth, Nathania Liem
Quebec City, QC
Dr. Catherine Mercier
Halifax, NS:
Drs Marilyn Mackay-Lyons, Anita Mountain
Charlottetown, PEI:
Drs Trish Helms-Neima, Nathanial Heinrichs
Target population:
Individuals within 5 days and 8 weeks of stroke who are experiencing hemiparesis requiring inpatient rehabilitation.
Recruitment:
The trial is currently recruiting participants. Target recruitment n = 120.
Eligibility:
Inclusion Criteria
- Primary ischemic anterior circulation stroke
- age ≥18 years
- at least 5 days after stroke but within 8 weeks of stroke on the date of medication (maraviroc or placebo) start
- hemiparesis requiring inpatient rehabilitation
- at least one of the following:
- some shoulder abduction, with gravity eliminated and visible extension in two or more digits
OR - visible hip flexion or extension
- some shoulder abduction, with gravity eliminated and visible extension in two or more digits
- assistance available for daily rehabilitation training practice and for transportation when needed
- adequate language skills to understand the Informed Consent and retain information during daily therapies
Exclusion Criteria
- pre-stroke modified Rankin score ≥ 2
- limited resources or illness that will not enable a return to living outside of a facility
- history of dementia
- history of hepatitis or elevated hepatic transaminases or bilirubin
- history of renal insufficiency or creatinine clearance (eGFR) < 60mL / min / 1.73m2
- cancer or other chronic illness that makes 1-year survival unlikely or will detract from the ability to carry out exercise and skills practice
- existing pre-stroke serious disabling disease (e.g., Parkinson’s disease, severe traumatic brain injury, amputation)
- seizure related to stroke
- acute or chronic epilepsy
- currently taking any of the following anticonvulsant medications:
- Carbamazepine, Phenobarbital, or Phenytoin
- pregnant, breastfeeding, or positive test for pregnancy at baseline
- women of childbearing potential who are not using one highly effective form of contraception or two forms of effective contraception
- known HIV positivity
- currently taking any of the following antifungal and/or antibacterial medications:
- Ketoconazole, Itraconazole, Voriconazole, Rifampin, Clarithromycin, or Rifabutin + Protease Inhibitor
- currently taking St. John’s Wort
Subgroup Stratification Criteria
For Upper Extremity Group:
Minimum Ability: Medical Research Council (MRC) grade >1 for shoulder abduction AND MRC grade >1 for finger extensor on at least one digit
Maximum Ability: Upper Extremity Fugl-Meyer Assessment Score >56
For Lower Extremity Group:
Minimum Ability: requiring a 2-person assist
Maximum Ability: walking speed <0.8m/s
Drs Ada Tang and Adria Quigley, pictured here, are the study leaders.
Description
Research studies in stroke recovery can help us better understand effective rehabilitation treatments to help reduce the burden of stroke.
Some groups of people however are often not as well represented in studies. For example, it is more common for men to take part in stroke research than women, and people with aphasia (a language impairment commonly seen after stroke) are often excluded from studies. Also, deciding whether to even take part in a research study can be difficult and overwhelming, especially in the early days after stroke, leaving many people to decline to participate.
Research has shown that women experience different barriers to participating in stroke research than men. This means that research findings, and the decisions made during stroke care based on these findings, may not reflect the true stroke population.
As researchers, we need to find better ways to help support groups like women and people with aphasia to participate in stroke research, so that study findings will better represent people living with stroke. In short, we need research on how to do research better.
With our pilot study, “Optimizing Recruitment to Drive Equitable Research opportunity in stroke rehabilitation trials in Canada” (ORDER-Pilot), we are taking the first steps in helping us understand how to optimize efficiency and quality in conducting clinical trials, and recruiting more diverse samples that are representative of the broader stroke population.
ORDER-Pilot is a ‘study-within-a-trial’, nested within Canadian Maraviroc RCT to Augment Rehabilitation Outcomes after Stroke (CAMAROS ; ‘host trial’). It will test the use of a supported, women-centred and aphasia-friendly recruitment and enrollment process for CAMAROS.
ORDER-Pilot also includes a substudy using survey and interviews to understand participants’ experiences of being approached by researchers to participate in CAMAROS.
Using a ‘study within a trial’ design, we are addressing important research gaps about the best tools for recruitment into trials, and understanding process factors such as participants’ perceptions of recruitment methods.
If ORDER-Pilot is feasible and potentially effective as a recruitment strategy for CAMAROS, we will have pilot evidence to support scale-up for future, larger trials on the CanStroke Recovery platform.
Sites involved
- Vancouver, BC
- Kelowna, BC
- Calgary, AB
- London, ON
- Toronto, ON
- Kingston, ON
- Windsor, ON
- Quebec City, QC
- Halifax, NS
- Charlottetown, PEI
Principal Investigators
Dr. Ada Tang, McMaster University
Dr. Adria Quigley, Dalhousie University
Other Investigators
Vancouver, BC:
Drs Janice Eng, Courtney Pollock
Kelowna, BC:
Dr. Brodie Sakakibara
Ms. Jennifer Monaghan, Patient Partner
Calgary, AB:
Drs Sean Dukelow, Michael Hill
Hamilton, ON:
Drs Jinhui Ma, Victrine Tseung
London, ON:
Dr. Robert Teasell
Toronto, ON:
Drs Mark Bayley, Susan Marzolini
Kingston, ON:
Drs Stephen Scott, Benjamin Ritsma
Windsor, ON:
Dr. Nathania Liem
Quebec City, QC
Dr. Catherine Mercier
Halifax, NS:
Dr. Marilyn Mackay-Lyons
Ms. Ferne Mardlin-Smith, Patient Partner
Target population
All individuals eligible for the CAMAROS trial will be eligible for the ORDER study, i.e. within 5 days and 8 weeks of stroke who are experiencing hemiparesis requiring inpatient rehabilitation.
Recruitment
The ORDER study is currently recruiting participants
Target recruitment n = 466
Study eligibility
Participants for the ORDER study will be all individuals eligible and approached for screening for the CAMAROS trial.
Internet-delivered cognitive behavioural therapy for persons with stroke: ICBT
Drs. Swati Mehta (left) and Robert Teassel (right) are the study Principal Investigators.
Description:
In Canada, stroke is a leading cause of adult disability. Along with the physical concerns, approximately 30% of people often experience symptoms of depression, but only 2- 3% access support. Unhelpful thoughts of never being able to go back to their life before their stroke and fear of recurring stroke can result in feelings of loss and hopelessness. If these thoughts go untreated over a long period of time, they can potentially lead to decreased quality of life and greater disability. Many of these individuals may benefit from access to mental health services, eg. cognitive behaviour therapy (CBT), that target maladaptive thoughts and behaviours. CBT is an evidenced based treatment strategy that helps patients recognize and challenge their unhelpful thoughts and behaviours that contribute to their mental health concerns. However, after stroke people often go untreated for various reasons, such as access to specialized care, costs, rural and remote location, lack of time, or concerns about stigma related to seeking care. One way to overcome these barriers is to provide these services over the internet. Internet delivered CBT (ICBT) has the potential for reaching a much wider group of people that may have unequal access to services.
Sites Involved:
- Canada-wide (Virtual)
Principal Investigator:
Swati Mehta, PhD Lawson Health Research Institute
Robert Teassel, MD St. Joseph’s Health Care London
Eligibility:
- Participants who have sustained a stroke and would like to learn strategies to improve their emotional well-being.
- The program is tailored to those with stroke that may have mobility and cognitive impairments.
Participant requirements:
Participants will be enrolled in an online 10-week program with potential guidance from a trained mental health clinician each week over the phone or through videoconferencing.
To learn more: swati.mehta@sjhc.london.on.ca
Dr. Sean Dukelow is the study Principal Investigator.
Robot-Enhanced Stroke Therapy Optimizes REhabilitation: RESTORE
Description:
Robotics in upper limb stroke rehabilitation first garnered attention in late 1990’s. Robots were a way to 1) perform passive range of motion and reduce hypertonia (resistance to passive movement), 2) aid patients in performing movements that would not otherwise be possible because of weakness and 3) increase strength by providing resistance to movements. The first observational study focused on chronic stroke and showed that working with a simple robotic device, the MIT-Manus, could improve motor function. Many observational studies using robotics for motor rehabilitation followed. As the number and complexity of robots increased, so did study designs.
Case-control and small single centre randomized controlled trials evaluated robotic therapy versus standard rehabilitation care or sham therapy. In most studies, robotic rehabilitation proved superior to the control conditions.
The purpose of this study is to investigate two aspects of robotic therapy after stroke. One goal is to determine if early robotic rehabilitation of the upper limb (beginning 5-9 days post-stroke) is more effective than later robotic rehabilitation (beginning 21-25 days post-stroke). The other goal is to determine if higher intensity robotic rehabilitation (2 hours/day) is more effective than lower intensity robotic rehabilitation (1 hour/day).
Sites Involved:
Calgary, AB
Kingston, ON
Principal Investigator
Dr. Sean Dukelow, MD, PhD, University of Calgary, Hotchkiss Brain Institute
Other Investigators:
Calgary, AB
Dr. Sean Dukelow
Kingston, ON
Drs Stephen Scott, Benjamin Ritsma
Target Population:
Individuals experiencing a recent first stroke who are experiencing an upper extremity impairment.
Recruitment:
The trial is currently recruiting participants.
Target recruitment n = 132 stroke participant, n=24 control participants.
Study Eligibility:
Inclusion Criteria – Stroke:
- Recent first stroke (ischemic or hemorrhagic)
- Upper extremity Fugl-Meyer score 15-45
- Modified Ashworth score of shoulder/elbow less than or equal to 2
- Able to follow task instructions
- Visual acuity better than 20/50 in both eyes
- Able to give consent
- Able to commit to follow-up
Inclusion Criteria – Control:
- Aged 18 or older
- Visual acuity better than 20/50 in both eyes
- Able to give consent
- Able to complete intervention
Exclusion Criteria:
- Prior stroke or significant neurologic problem (e.g. Multiple Sclerosis)
- Pre-existing musculoskeletal injury that will interfere with active therapy
- Pre-Stroke Modified Rankin Score > 2
- Clinical evidence of Unilateral Spatial Neglect on the Behavioural Inattention Test (BIT)
- Enrollment in a concurrent clinical intervention trial
- Major co-morbid or concurrent illness such that improvement is unlikely or completion of the protocol as specified is unlikely
Drs Brodie Sakakibara and Ada Tang are the study Principal Investigators.
TeleRehabilitation with Aims to Improve Lower Extremity Recovery Post-Stroke: TRAIL
TRAIL Randomized Controlled Trial (TRAIL-RCT)
Description:
The multi-site RCT aims to compare functional mobility between stroke survivors in TRAIL, a 4-week progressive intensity and self-management support telerehabilitation program, and those in the attention-controlled stroke education program (EDUCATION). The trial also compares lower extremity muscle strength, motor impairment, functional balance, balance self-efficacy, and costs and health-related quality of life between TRAIL and EDUCATION participants.
The end goal is to inform best practices in virtual care and have widespread application in practice when access to in-person rehabilitation is not feasible, such as in rural, remote and under-serviced areas.
Sites involved:
- Vancouver
- Kelowna
- Winnipeg
- Halifax
- Toronto
- London
Principal Investigators:
Dr. Ada Tang, McMaster University
Dr. Brodie Sakakibara, University of British Columbia, Okanagan
Other investigators:
- Nova Scotia Health Authority (Halifax), site investigator Dr. Marilyn Mackay-Lyons,
- University Health Network (Toronto), site investigator Dr. Mark Bayley,
- Parkwood Institute (London), Dr. Robert Teasell,
- Riverview Health Centre (Winnipeg), Dr. Ruth Barclay & Dr. Sepideh Pooyania,
- GF Strong Rehabilitation Centre (Vancouver), Dr. Courtney Pollock.
- McMaster University (Hamilton), Elise Wiley, PhD candidate
- Patient Partner, Jennifer Monaghan
Target population for the trial:
Individuals within 12 months of stroke who are experiencing lower extremity impairment.
Recruitment:
The trial is currently recruiting participants
Target recruitment n=96 (n=48 females, 48 males)
Study eligibility:
Inclusion Criteria:
- ≥19 years of age
- ≤12 months post-stroke with lower extremity hemiparesis
- Walk ≥10 meters with or without a gait aid and without physical assistance of another person
- Tolerate 50 minutes of activity (including rest breaks)
Exclusion Criteria:
- Currently participating in formal in- or out-patient stroke rehabilitation focusing on lower extremity training
- Living in long-term care
- Severe vision or hearing loss
- Significant musculoskeletal or other neurological conditions
- Not medically stable
- Comorbidities (e.g. limb amputation), pain or other symptoms that significantly impact lower extremity
To learn more: info@canadianstroke.ca
Telerehabilitation with Aims to Improve Lower Extremity Recovery – Proof-of-Concept (TRAIL-PROOF)
The TRAIL-RCT was preceded by a proof-of-concept study, TRAIL-PROOF.
Description:
TRAIL-Proof was a feasibility study aiming to examine the feasibility of a 4-week lower extremity telerehabilitation program to improve lower extremity recovery among community-living stroke survivors across Canada. Thirty-two patients have been enrolled in the study at 5 Canadian sites.
Participants received a telerehabilitation program comprised of evidence-based exercises and self-management delivered by physiotherapist trained in telerehabilitation over videoconferencing. The program consisted of two 60-minute telerehabilitation sessions per week over the course of 4 weeks. Participants were also asked to complete at least one additional independent self-managed exercise session each week. Study participants were evaluated before the start of the telerehabilitation program and immediately after the telerehabilitation program.
Sites involved:
University of British Columbia & GF Strong Centre, Vancouver, British Columbia
Riverview Health Centre, Winnipeg, Manitoba
Dalhousie University, Halifax, Nova Scotia
Parkwood Institute, London, Ontario
Toronto Rehabilitation Institute – University Health Network, Toronto, Ontario
Principal Investigators:
Brodie Sakakibara, PhD
Ada Tang PT PhD
Other Investigators:
Mark Bayley, MD. University Health Network, Toronto
Courtney Pollock, PhD. University of British Columbia & Rehabilitation Research Program
Janice Eng, PhD. University of British Columbia & Rehabilitation Research Program
Sepideh Pooyania, MD. Riverview Health Centre
Ruth Barclay, PhD. Riverview Health Centre
Marilyn Mackay-Lyons, PhD. Dalhousie University
Robert Teasell, MD. Parkwood Institute
Sarah Park, MSc, University of British Columbia & Rehabilitation Research Program
TRAIL Publications
May 24, 2024 Associations between balance self-efficacy and virtual balance performance
Examining the association between balance self-efficacy and virtual balance performance in individuals with stroke: a cross-sectional study
Authors: Eric Huynh, Elise Wiley, Sarah Park, Brodie M Sakakibara, Ada Tang
Published in Top Stroke Rehabil. 2024 May 24:1-9. doi: 10.1080/10749357.2024.2356407. Online ahead of print.
Link to paper https://www.tandfonline.com/doi/full/10.1080/10749357.2024.2356407
March 1, 2024 Results from TRAIL Proof of Concept Study
Investigating the Telerehabilitation With Aims to Improve Lower Extremity Recovery Poststroke Program: A Feasibility Study
Authors: Sarah Park, Ada Tang, Ruth Barclay, Mark Bayley, Janice J Eng, Marilyn Mackay-Lyons, Courtney Pollock, Sepideh Pooyania, Robert Teasell, Jennifer Yao, Brodie M Sakakibara
Published in Phys Ther. 2024 Mar 1;104(3):pzad165. doi: 10.1093/ptj/pzad165.
Link to paper: https://pubmed.ncbi.nlm.nih.gov/38051660/
February 15, 2024 Qualitative study of participant experiences of TRAIL
Exploring the experiences of an exercise-based telerehabilitation program among Canadian community-dwelling adults with stroke
Authors: Elise Wiley, Brodie Sakakibara, Sarah Park, Ruth Barclay, Mark Bayley, Janice J Eng, Anne Harris, Elizabeth Inness, Marilyn MacKay-Lyons, Joy MacDermid, Courtney Pollock, Sepideh Pooyania, Robert Teasell, Jennifer Yao, Ada Tang
Published in Disabil Rehabil. 2024 Feb 15:1-11. doi: 10.1080/09638288.2024.2316772. Online ahead of print.
Link to paper https://www.tandfonline.com/doi/full/10.1080/09638288.2024.2316772
July 19, 2023 Protocol for TRAIL Randomized Controlled Trial
TeleRehabilitation with Aims to Improve Lower extremity recovery in community-dwelling individuals who have had a stroke: protocol for a multisite, parallel group, assessor-blinded, randomised attention-controlled trial
Authors: Brodie M Sakakibara, Elise Wiley, Ruth Barclay, Mark Bayley, Jennifer C Davis, Janice J Eng, Anne Harris, Elizabeth L Inness, Marilyn MacKay-Lyons, Jennifer Monaghan, Courtney Pollock, Sepideh Pooyania, Amy Schneeberg, Robert Teasell, Jennifer Yao, Ada Tang
Published in BMJ Open. 2023 Jul 19;13(7):e076723. Doi: 10.1136/bmjopen-2023-076723.
Link to paper: https://bmjopen.bmj.com/content/13/7/e076723.long
TRAIL In the News
28 March 2024 UBC Okanagan News, Virtual rehabilitation provides benefits for stroke recovery https://news.ok.ubc.ca/2024/03/28/virtual-rehabilitation-provides-benefits-for-stroke-recovery/
July 10, 2022 Vancouver Coastal Health Research Institute article, Making lower body rehabilitation more accessible to stroke patients https://www.vchri.ca/stories/2022/07/10/making-lower-body-rehabilitation-more-accessible-stroke-patients
19 January 2022 Interview with UK-based NR Times, TRAIL study brings new remote rehab potential to stroke survivors https://nrtimes.co.uk/trail-study-brings-new-remote-rehab-potential-to-stroke-survivors/
Dr. Janice Eng is the study Principal Investigator.
Virtual Physical Activity Seated Exercise Study: V-PASE
Description:
The Virtual Physical Activity Seated Exercise (V-PASE) study is a 10-week online exercise study in those living with a stroke and mobility impairment. The study has the potential to improve an individual’s balance, mobility, muscle strength, quality of life, and heart health (sugar and cholesterol levels).
The study is conducted in multiple provinces across Canada with all sessions being completed online (e.g., Zoom) in the comfort of your own home. Intensive seated exercise sessions will be delivered by a trained instructor or physical therapist and will be 60 minutes in duration and take place 3 times per week.
Who can join this study?
- Adults who have been living with stroke more than 6 months
- Live in BC, Saskatchewan, Manitoba, Ontario, or Nova Scotia
- Have ongoing walking and standing issues due to their stroke
- Use a walking device such as a cane or walker in large indoor spaces (e.g., shopping mall) or outdoor spaces, and
- Able to stand up from a chair.
Principal Investigator:
Dr. Janice Eng, University of British Columbia
Other investigators:
British Columbia – Dr. Paul Mackie | Dr. Jennifer Yao | Dr. Ben Mortenson | Sally-Anne Stelling | Dr. Courtney Pollock | Dr. Maureen Ashe | Dr. Brodie Sakakibara
Saskatchewan – Dr. Sarah Donkers
Manitoba – Dr. Ruth Barclay | Dr. Sepideh Pooyania
Ontario – Dr. Sue Peters | Dr. Mark Bayley
Nova Scotia – Dr. Adria Quigley
Target population for the trial:
Adults living with a stroke for more than 6 months and have a mobility impairment (walking difficulties that require a walking device in outdoor spaces or large indoor areas).
Access to a local blood facility for sugar and cholesterol lab work is needed. We can work with local health authorities to schedule blood work.
Recruitment:
The trial is currently recruiting patients in all Provinces listed above.
To learn more: info@canadianstroke.ca
Dr. Mark Bayley is the study Principal Investigator.
Exploring Methods to improve Participation Of Women in clinical trials to Help Enhance stroke Recovery research: EMPOW-HER
Description:
Sex differences exist in the burden of stroke and treatment efficacy, therefore equal representation in research studies is of paramount importance. However, women are under-represented in stroke research trials reducing the generalizability of research outcomes.
Therefore, we are conducting two cross-sectional questionnaire-based studies and one focus group to determine sex and gender-related factors associated with willingness to participate in stroke research studies. A retrospective review of CanStroke Recovery Trials data is also underway, to determine whether the sex distribution as well as other demographic and clinical characteristics of participants differed from that of the general diseased population.
Sites Involved:
A survey of the CanStroke research team will be sent to all current CanStroke personnel to explore their perceptions of barriers and facilitators to recruitment of women and men in clinical trials.
Respondents for the survey of people post-stroke will be recruited from 9 sources across Canada. These include in-patient and out-patient stroke rehabilitation programs, cardiovascular rehabilitation, and March of Dimes.
We will also be contacting the CanStroke Trials Recovery Platform researchers to invite them to disseminate research flyers to the patients of their studies.
Principal Investigator:
Dr. Mark Bayley, MD
Other Investigators:
Dr. Susan Marzolini
Dr. Shannon MacDonald
Dr. Urvashy Gopaul
Dr. Amy Yu
Juliana Nunes da Silva
And others from the CanStroke research team.
Target population:
The CanStroke Recovery Trials research team.
Men and women post-stroke.
Recruitment:
Recruitment is underway for the cross-sectional questionnaire of people post-stroke (target of 400 respondents).
Study eligibility:
Men and women (at least 18 years of age) having had at least one stroke (any type).
Ability to read in English.
Dr. Sean Dukelow is study Principal Investigator.
Description
VIsion and Proprioception Evaluation with Robotics after Stroke (VIPERS) will assess vision and proprioceptive impairments after stroke using eye tracking software on the KinArm Exoskeleton.
Recruitment will be underway in the Fall of 2025 from sites in Calgary, AB, Toronto, ON, Kingston, ON, and Quebec City, QC.
The published study can be found HERE.
Description:
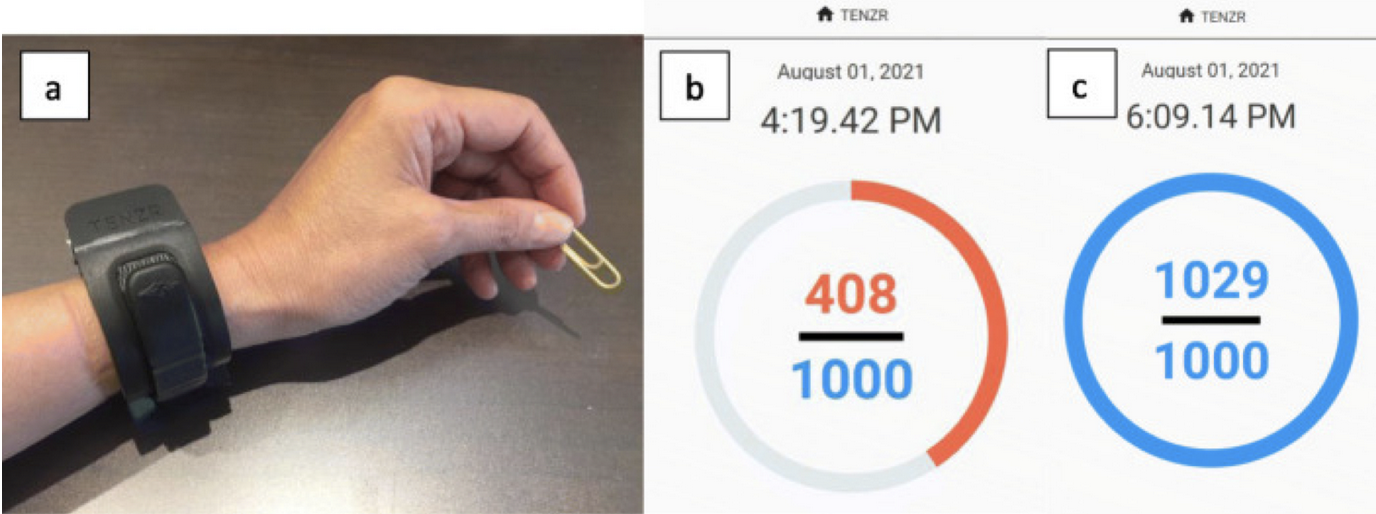
This study examines the feasibility and effect of a program that combines exercise and feedback from a wearable device on upper limb movement practice and function in individuals with stroke.
Participants were randomized into either the Immediate Treatment Group or the Delayed Treatment group. Both groups completed the same intervention program. The Immediate treatment group started the program right away while the Delayed Treatment group started the program after a 3-week delay.
The intervention program is 3 weeks in duration and consists of participants completing at least two hours of exercises (adapted from the Home-GRASP program) daily and wearing an activity monitor on their affected wrist during waking hours for the duration of the intervention. Participants were asked to meet daily movement count goals based on information from the monitor and had 6 virtual sessions with a therapist.
Sites involved:
- GF Strong Rehabilitation Centre
- Foothills Medical Centre
- Riverview Health Centre
- Parkwood Institute
- Sunnybrook Health Sciences
- UHN-Toronto Rehabilitation Institute
- Nova Scotia Rehabilitation and Arthritis Centre
Principal Investigator:
Dr. Janice Eng, University of British Columbia
Other investigators:
Dr. Sean Dukelow (Calgary, AB)
Dr. Ruth Barclay (Winnipeg, MB)
Dr. Bob Teasell (London, ON)
Dr. Bradley MacIntosh (Toronto, ON)
Dr. Mark Bayley (Toronto, ON)
Dr. Marilyn MacKay-Lyons (Halifax, NS)
Target population:
Adults living with a stroke less than one year and have a mobility impairment on stroke affected upper limb
Recruitment:
Data collection has been completed. 73 participants were enrolled in the study.
Study eligibility:
- 19 years or older
- Less than 1 year since the stroke occurred
- Living in the community
- Have unilateral upper limb impairment
- Have some ability to move their arm and hand (> 30° shoulder flexion or abduction and Fugl Meyer finger extension score > 0)
- Are using their affected upper limb in a different way than prior to their stroke (REACH score < 4)
- Completed formal physical and occupational therapy rehabilitation for the upper limb
- Have access to a tablet, computer, laptop or phone with internet and email access.
The trial protocol is published at the following site:
https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-022-06047-9
FLuoxetine to Open the critical time period Window to improve motor recovery after stroke: FLOW
Description:
FLOW Trial is a randomized, placebo-controlled, blinded phase II trial evaluating the efficacy of coupling antidepressant therapy (e.g., selective serotonin reuptake inhibitor – fluoxetine) with exercise rehabilitation in expanding the window of post-stroke recovery and improving functional outcomes. 52 patients have been enrolled in the study at 8 Canadian sites.
Participants were randomized into the intervention and the control group. The intervention group received a low dose of active drug fluoxetine, while the control group received placebo. Both groups received a 12-week, 3 times per week exercise program in addition to standard of care rehabilitation. Study participants were evaluated at baseline, post-exercise program and 6-months post-exercise program.
Sites Involved:
- University of Calgary, Calgary, Alberta,
- University of British Columbia & GF Strong Centre, Vancouver, British Columbia
- Riverview Health Centre, Winnipeg, Manitoba,
- Memorial University of Newfoundland, St. John’s, Newfoundland and Labrador
- Dalhousie University, Halifax, Nova Scotia,
- Parkwood Institute, London, Ontario
- Sunnybrook Health Sciences Centre, Toronto, Ontario
- Toronto Rehabilitation Institute – University Health Network, Toronto, Ontario
Principal Investigators:
Dr. Mark Bayley and Dr. Janice Eng
Other Investigators:
Dr. Mark Bayley, MD. University Health Network, Toronto
Dr. Courtney Pollock, PhD. University of British Columbia & GF Strong Rehab Centre
Dr. Bradley MacIntosh, PhD, Sunnybrook Health Sciences Centre
Dr. Sean Dukelow, MD, PhD, University of Calgary/Hotchkiss Brain Institute
Dr. Sepideh Pooyania, MD. Riverview Health Centre
Dr. Michelle Ploughman, PhD. Memorial University of Newfoundland
Dr. Marilyn Mackay-Lyons, PhD. Dalhousie University
Dr. Robert Teasell, MD. Parkwood Institute
Dr. Marc Roig, McGill, University, Quebec
Target Population:
Individuals within 12 months of stroke who are experiencing lower extremity impairment.
Recruitment:
The trial is not recruiting patients. Recruitment and data collection have been completed and researchers have begun analysis of the results.
Eligibility:
Inclusion Criteria:
- 25 years of age or older
- Between 2 to 12 months post-stroke
- Experiencing significant weakness in one or both legs as the result of stroke
- Not currently taking SSRIs or MOIs
Exclusion Criteria:
Pregnancy
Pre-existing conditions causing severe impairment of mobility
Taking medications for depression
Substantial premorbid disability or pre-existing deficit or language comprehension deficit that could interfere with assessments
Unstable serious medical condition (e.g., terminal cancer, renal or liver failure, congestive heart failure)
Uncontrolled high blood pressure
Requires more than a one person assist for transfer
Planned surgery that would affect participation in the trial
Participating in another formal lower limbs exercise program more than one day per week
History of seizures
Modafinil and Exercise for Post Stroke Fatigue: MODEX
Description:
A lot of people report fatigue as one of the worst symptoms post stroke that can affect daily activities and the length and quality of life. We do not fully understand all the reasons for fatigue after stroke or how to best treat it. We think that fatigue results from the stroke changing the brain, reducing physical fitness, and decreasing muscle strength.
Some studies have tested a drug called Modafinil for post stroke fatigue, while other studies have tested exercise for it. Yet, there is unclear evidence for either treatment so our study has two main aims:
- Test which type of exercise is best.
- Test if Modafinil is better than a sugar pill.
As another aim, we will also look at if combining Modafinil with exercise has any benefits.
We will assess the results to identify the best treatment for post stroke fatigue. We hope to be able to find a treatment that will help reduce fatigue and improve quality of life after a stroke.
Sites Involved:
- Toronto (UHN and Sunnybrook)
- London, ON
- Vancouver
- Calgary
- Winnipeg
- Halifax
- St. John’s
Principal Investigators:
Dr. Mark Bayley, MD
Dr. Janice Eng, PhD
Other Investigators:
Dr. Mark Bayley, Toronto Rehabilitation Institute, University Health Network
Drs. Bradley MacIntosh and Sandra Black, Sunnybrook Health Sciences Centre
Dr. Sean Dukelow, University of Calgary
Drs. Jennifer Yao, Janice Eng, and Courtney Pollock, University of British Columbia & GF Strong Rehab Centre
Drs. Michelle Ploughman and Jason McCarthy, Memorial University of Newfoundland
Drs. Marilyn Mackay-Lyons and Anita Mountain, Dalhousie University
Dr. Robert Teasell, Parkwood Institute
Drs. Sepideh Pooyania and Ruth Barclay, Riverview Health Centre
Target Population:
Individuals with fatigue > 3 months post stroke.
Recruitment:
Not recruiting yet.
Target number: up to n=300.
Vision and Proprioception Evaluation with Robotics after Stroke: VIPERS
Description:
Vision is the sense of being able to see. Proprioception is the sense of where the limbs or body are in space. Approximately two-thirds of stroke survivors have problems with vision and half have problems with proprioception. Impairments in these senses lead to difficulties performing daily tasks and longer hospital stays. At the bedside, clinicians tend to use crude measurements of vision and proprioception. For vision, clinicians may have the patient attempt to track the clinician’s finger to test eye movements and get the patient to count fingers to measure visual fields. For proprioception, clinicians often ask the patient to close their eyes and then passively move the patient’s finger up or down and ask which direction it was moved in. Our team has spent many years developing and validating more precise, reliable measures of proprioception using robotics. We recently integrated eye tracking technology into our robots.
The current project revolves around improving our understanding of visual and proprioceptive loss after stroke and its impact on reaching movements using these technologies. We are particularly interested in examining the integration of vision and proprioception and the brain regions responsible for these senses. We plan to recruit stroke survivors within the first few days post-stroke and they will complete a series of automated robotic assessments of vision and proprioception over the following 6 months, alongside several routine clinical assessments. We will also recruit healthy individuals to develop normative datasets. Study participants will complete brain MRI’s (magnetic resonance images) which will allow us to better understand how different types of brain damage from stroke impact the recovery of vision and proprioception. We believe improving our understanding of this will allow us to develop better and more personalized therapies for stroke survivors.
Sites Involved:
- Calgary, AB
- Toronto, ON
- Kingston, ON
- Quebec City, QC
Recruitment:
Not recruiting yet. Recruitment will be underway in the Fall of 2025 .
brAin coNtrolled robotic arM rehabilitation fOr stRoke: ANIMATOR
Description
Every day we make hundreds of reaches to all sorts of objects. After a stroke, as many as 80% of stroke survivors have difficulty doing this. A key treatment is rehabilitation which focuses on repetitive, task-specific activities to engage neuroplastic mechanisms in the brain to “rewire” circuits responsible for arm and hand movement. However, success with this approach is limited, especially if the individual has very limited limb movement. A severely impaired arm is devastating as most activities of daily living require the use of two arms (e.g., dressing). The use of brain computer interfaces (BCI) to control robotic rehabilitation tools has high potential to change this. With the use of a cap containing surface electrodes worn on the head, and a computer laptop that employs machine learning algorithms, it is possible for a stroke survivor to control a robotic device that can animate the stroke affected arm. This allows individuals with little-to-no active arm movement to undertake task-specific therapies and harness neuroplastic mechanisms necessary to bring about changes in the brain. The intervention takes a precision medicine approach to rehabilitation as BCI can adapt to different types of brain damage as well as variations in an individual’s brain activity as they go through the recovery process.
This novel-therapeutic approach may finally represent an effective therapeutic option for the thousands of Canadians currently suffering with severe arm impairment because of their stroke. We have assembled an experienced, diverse team of researchers, clinicians, and a person with lived experience to examine the ability of a BCI robotic device, RehUp, produced by a Canadian BioTech company VIBRAINT Inc, to improve arm function in individuals with chronic, severe post-stroke arm impairment.
Sites Involved:
- Calgary, AB
- Toronto, ON
- Vancouver, BC
Principal Investigators:
Dr. Sean Dukelow, University of Calgary
Other Investigators:
Dr. Janice Eng, University of British Columbia
Dr. Mark Bayley, Toronto Rehabilitation Institute, University Health Network
Dr. Michael Hill, University of Calgary
Recruitment:
Not recruiting yet.
STroke Recovery wIth Virtual rEality: STRIVE
Description
Stroke rehabilitation in Canada is approaching a crisis point. Rising stroke incidence, improved acute care survival, and stagnant rehabilitation staffing have created overwhelming pressure on an already strained healthcare system. Many stroke survivors – especially those in rural and remote areas – cannot access the intensity (frequency or duration) and quality of therapy needed to optimize their recovery. One-to-one therapist models and geographic barriers are limiting recovery potential for the more than 5,000 Albertans who experience a stroke each year.
This project proposes the use of immersive Virtual Reality (VR) to extend expert-level stroke rehabilitation into the home and under the supervision of therapists. The team has already developed and clinically tested VR modules targeting lower body, upper limb and visuospatial recovery. The team will refine these modules for home-based use based on the needs of the Calgary Stroke Program, optimize our clinician interface to track therapy and progress, and co-develop a novel VR module focused on post-stroke aphasia. The aphasia tool will integrate Red Iron Labs’ large language models and AI-guided therapy (using their Canadian data servers and custom data models) to support communication recovery where speech-language resources are lacking.
Two pilot studies will evaluate feasibility, usability, and early outcomes—one focused on motor/visual-spatial recovery, the other on aphasia. The project brings together clinicians, stroke survivors, and developers in a user-centered design process, ensuring real-world fit and uptake.
Our long-term goal is a scalable, data-driven, Health Canada–compliant VR solution that allows clinicians to direct rehabilitation remotely, improving therapy dose and extending access to patients who would otherwise go without. This project will generate the evidence needed to support a national randomized trial and, ultimately, sustainable adoption within Alberta’s health system.
Sites Involved:
- Calgary, AB
Principal Investigators:
Dr. Sean Dukelow, University of Calgary
Recruitment:
Not recruiting yet.
CanStroke Recovery Trials platform welcomes both academic and industry trials. New trials are evaluated by the management team and Steering Committee based on relevance, potential impact, and capacity.